19/10/2019
Acute inguinal hernias represent a common surgical emergency, and while surgical intervention is often the ultimate solution, the role of non-operative management, specifically 'taxis', is gaining attention. Taxis, a technique involving manual reduction of a hernia under analgesia or sedation, offers a potential first-line treatment, particularly in situations where immediate surgical care might be limited or when delaying surgery is beneficial for the patient. This article delves into the nuances of taxis in the context of emergency inguinal hernias, examining its effectiveness, safety, and appropriate application based on current literature.

- Understanding Inguinal Hernias and the Need for Taxis
- The Literature on Taxis: Evidence and Findings
- When to Consider Taxis: Indications and Contraindications
- The GPS Taxis Technique: A Safe Approach
- Analgesia and Sedation: Optimising Patient Comfort and Safety
- Outcomes and Future Directions
- Conclusion
Understanding Inguinal Hernias and the Need for Taxis
An inguinal hernia occurs when tissue, such as part of the intestine, protrudes through a weak spot in the abdominal muscles of the groin. When this protruding tissue cannot be pushed back into the abdomen, it is termed an 'incarcerated' hernia. If the blood supply to the incarcerated tissue becomes compromised, it escalates to a 'strangulated' hernia, a critical condition requiring urgent surgical intervention. The increase in emergency presentations of inguinal hernias, partly due to 'watch and wait' policies for less acute cases, highlights the importance of understanding all available management options. Guidelines from organisations like HerniaSurge and WSES have begun to address emergency groin hernias, but the specific role of taxis has often been overlooked.
The primary benefit of taxis lies in its potential to avoid or delay immediate surgery. This is particularly relevant for elderly patients with comorbidities or those on anticoagulant therapy, where the risks of emergency surgery might be higher. Furthermore, in the context of global health challenges like the COVID-19 pandemic, where healthcare systems can be overwhelmed and the risk of anaesthesia for patients may be increased, taxis emerges as a valuable adjunct to care. It allows for the possibility of deferring definitive surgical repair until a more opportune and safer time, potentially weeks later.
The Literature on Taxis: Evidence and Findings
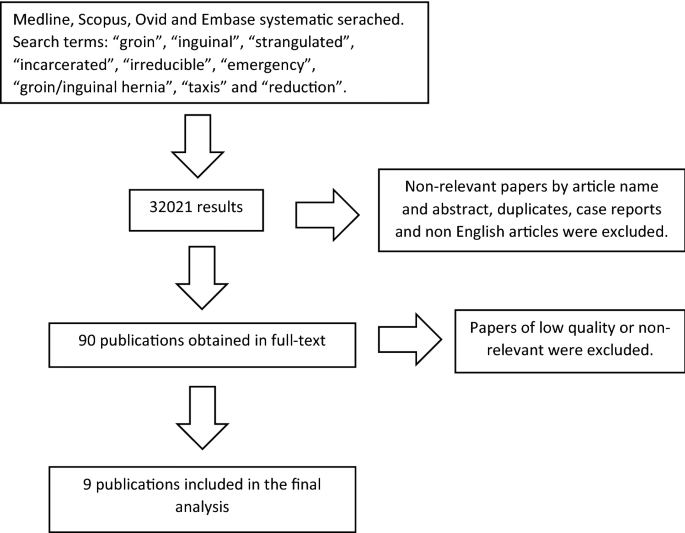
A review of available literature, encompassing databases like Medline, Scopus, Ovid, and Embase, sought to assess the role of taxis in emergency inguinal hernias. Despite an initial large number of identified papers, only a select few met the criteria for inclusion due to varying methodologies and definitions. A significant challenge identified was the inconsistent terminology used to describe incarcerated versus strangulated hernias, making a precise separation difficult in analysis. However, the literature suggests that taxis can be safely attempted early in the symptom presentation of an incarcerated inguinal hernia. Studies indicate a success rate of approximately 70% in patients where taxis is attempted. It is crucial to be aware of the potential for 'reduction en masse', a rare complication where the hernia contents are reduced, but the sac remains incarcerated within the abdominal wall. If taxis is successful, definitive surgical repair can be scheduled electively, either during the same hospital admission or within a month, depending on patient and hospital circumstances.
The effectiveness of taxis appears to be inversely related to the duration of symptoms. The longer the hernia has been incarcerated, the lower the chance of successful manual reduction. While the risk of strangulation and the need for bowel resection increase with time, with some studies suggesting the risk doubles for every 24 hours of delay, it's important to note that not all incarcerated hernias progress to strangulation. The presence of infarcted bowel within the hernia is a definitive contraindication for taxis.
When to Consider Taxis: Indications and Contraindications
The primary contraindication for attempting taxis is the presence of clinical signs strongly suggestive of strangulated bowel within the hernia. These signs may include:
- Tachycardia
- Hypotension
- Peritonitis
- Localised signs of inflammation over the hernia, such as erythema (redness) and extreme tenderness to touch.
In the absence of these definitive signs of strangulation, taxis can be considered. Even symptoms of bowel obstruction, without the aforementioned localised or systemic signs, do not necessarily preclude an attempt at taxis. It is vital to differentiate from other groin swellings, such as abscesses, testicular torsion (a surgical emergency itself), or enlarged lymph nodes.
The time elapsed since the onset of symptoms is a critical factor. While a precise cutoff is difficult to define, hernias present for less than 24 hours with minimal localised signs are generally better candidates for taxis. Beyond 24 hours, the risk of strangulation and ischaemia increases significantly, making surgical intervention a more prudent choice. However, each case must be assessed individually.
The GPS Taxis Technique: A Safe Approach
A structured approach to performing taxis, termed 'GPS Taxis', emphasizes three key elements for safe and effective manual reduction:
G – Be Gentle
This involves applying steady, gentle pressure over the hernia for a sustained period (5-15 minutes) rather than forceful manipulation. The aim is to encourage the incarcerated contents to return to the abdominal cavity through the hernial ring, rather than pushing them against it.
P – Be Prepared
This signifies the importance of an appropriate clinical environment and preparedness for potential complications. This includes:
- Ensuring adequate resuscitation measures are in place.
- Administering oxygen therapy.
- Establishing intravenous access and monitoring vital signs (oxygen saturation, heart rate).
- Creating a calm environment, away from distracting noise.
- Positioning the patient appropriately, potentially in Trendelenburg.
- Having anaesthetists present, especially for frail or elderly patients.
S – Be Safe
Safety is paramount. If strangulation is suspected, taxis should not be attempted. When performing taxis, the smallest effective dosage of analgesia and sedation should be used. This involves careful titration of intravenous medications. A common and effective regimen involves a combination of intravenous morphine for pain relief and a short-acting benzodiazepine, such as midazolam, for sedation. The drugs should be administered slowly, titrating to the patient's response, and it's crucial to be aware of their onset of action and potential side effects. Reversal agents like naloxone for opioids and flumazenil for benzodiazepines should be readily available.
Analgesia and Sedation: Optimising Patient Comfort and Safety
The conscious sedation used during taxis aims to reduce pain and promote relaxation. While traditional regimens included diazepam and morphine, midazolam with morphine is now more commonly favoured due to midazolam's faster and shorter action. It is vital to administer these drugs intravenously, titrating them carefully. Typical doses might involve 5-10 mg of morphine and 2.5-5 mg of midazolam, but these must be individualised based on the patient's condition, especially in the elderly or those with comorbidities. Close monitoring of the patient's level of consciousness and respiratory status is essential throughout the procedure and into the recovery period, as the effects of the sedatives can persist. Patients should be advised to seek immediate medical attention if symptoms of bowel ischaemia or obstruction recur.
Outcomes and Future Directions
Successful taxis can lead to the deferral of surgery, allowing for elective repair at a later, more convenient, and potentially safer time. This approach can significantly reduce the need for emergency operations, particularly in resource-limited settings or during public health crises. However, the inconsistency in terminology and methodology across studies presents a limitation in drawing definitive conclusions and performing meta-analyses. Future research with clearer definitions and standardised reporting is needed to further elucidate the role and optimal application of taxis in the management of acute inguinal hernias. The establishment of an international registry could provide valuable data on the incidence, complications, and long-term outcomes associated with taxis.
Conclusion
Taxis offers a safe and effective non-operative option for the initial management of acute inguinal hernias, especially when strangulation is unlikely. Its utility is amplified in situations where immediate surgical access is challenging or when delaying surgery is medically advantageous for the patient. By adhering to the principles of the GPS Taxis technique and employing careful patient assessment and sedation, clinicians can leverage this historical yet relevant procedure to improve patient outcomes and optimise the use of healthcare resources, particularly in times of increased demand on surgical services.
Frequently Asked Questions about Taxis for Inguinal Hernias:
Can taxis be used in emergency inguinal hernia surgery?
Taxis itself is not surgery, but a method to attempt to manually reduce the hernia contents back into the abdomen. It can be used as a first-line treatment before surgery, potentially delaying or avoiding the need for emergency surgery, especially if surgical care is not immediately available or if the patient is not fit for immediate surgery. Definitive surgical repair can then be arranged later.
How effective is taxis in reducing an acute inguinal hernia?
Studies suggest that taxis can be effective in approximately 70% of patients with an incarcerated inguinal hernia, provided there are no signs of strangulation. The success rate is generally higher when attempted earlier in the course of symptoms.
What are the risks associated with taxis?
The main risks include failure to reduce the hernia, and the rare complication of 'reduction en masse'. If strangulation is present, attempting taxis can delay definitive treatment. Complications related to sedation, such as respiratory depression or hypotension, can also occur if not managed carefully.
When should taxis NOT be attempted?
Taxis should not be attempted if there are clinical signs of strangulation, such as severe pain, localised inflammation (redness, heat), fever, tachycardia, hypotension, or signs of peritonitis. If the hernia contains non-viable bowel, taxis is contraindicated.
What is the recommended sedation for taxis?
Conscious sedation is typically used, often with a combination of intravenous opioids (like morphine) for analgesia and a benzodiazepine (like midazolam or diazepam) for sedation. The drugs should be titrated carefully to the lowest effective dose, and the patient's vital signs monitored closely.
Can a hernia be reduced by a taxi (vehicle)?
No, the term 'taxis' in this context refers to the medical procedure of manual reduction, not a vehicle. The word originates from the Greek word for 'arrangement'.
Is taxis a suitable treatment option during the COVID-19 pandemic?
Yes, taxis can be a useful adjunct during pandemics like COVID-19. It can help reduce the number of patients requiring immediate hospital admission and surgery, thereby minimising exposure risks for both patients and healthcare workers, and easing the strain on healthcare services.
If you want to read more articles similar to Taxis: A Gentle Approach to Inguinal Hernias, you can visit the Taxis category.